
Case Report | DOI: https://doi.org/10.31579/2578-8868/159
1* Department of Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, Kings College London
*Corresponding Author: Modhi A Alhussinan, Department of Neuroscience, Institute of Psychiatry, Psychology and Neuroscience, Kings College London
Citation: Modhi A Alhussinan., (2021) Limbic system. J. Neuroscience and Neurological Surgery. 8(3); DOI:10.31579/2578-8868/159
Copyright: © 2021 Modhi A Alhussinan, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited
Received: 02 February 2021 | Accepted: 22 March 2021 | Published: 26 March 2021
Keywords: human brain;limbic system; neurological diseases
The limbic system forms a crucial part of the human brain. It is a network of structures that set beneath temporal lobe and on both sides of thalamus. It has a wide range of functions which mainly involve in our behavioral and emotional responses. Therefore, any disruption to the system may lead to devastating neurological conditions. This essay will explore the structure of the limbic system, its functional organization utilizing neurological diseases or damage to demonstrate the association between that specific affected brain region and function.
The limbic system forms a crucial part of the human brain. It is a network of structures that set beneath temporal lobe and on both sides of thalamus. It has a wide range of functions which mainly involve in our behavioral and emotional responses. Therefore, any disruption to the system may lead to devastating neurological conditions. This essay will explore the structure of the limbic system, its functional organization utilizing neurological diseases or damage to demonstrate the association between that specific affected brain region and function.
The concept of limbic system has a historical value in the field of neuroscience despite the lack of consensus concerning the exact structures forming the limbic system (Kötter & Meyer, 1992)(Pessoa & Hof, 2015). In 1878, Paul Pierre Broca refer to the great limbic lobe located at the edge of the cerebral cortex as “limbic” (limbus for border in Latin). Furthermore, in 1937, James Papez has proposes an anatomical model known as Papez circuit followed by Yakovlev's circuit in 1948, and finally MacLean who formulated the term “Limbic System” (RajMohan & Mohandas, 2007) (Vogt, 2019).
Knowledge expansion in the last few decades enriched us with a wealth of information about the connectivity and function of the limbic system. It is perceived as a set of brain regions that is situated in the medial aspect of the brain and highly interconnected. These regions include: the orbitofrontal cortex, insular cortex, anterior and posterior cingulate cortices, temporopolar cortex, parahippocampal gyrus, hippocampal formation, amygdala, basal forebrain, anterior thalamic nuclei, and the hypothalamus (Purves et al., 2001) (Figure1).
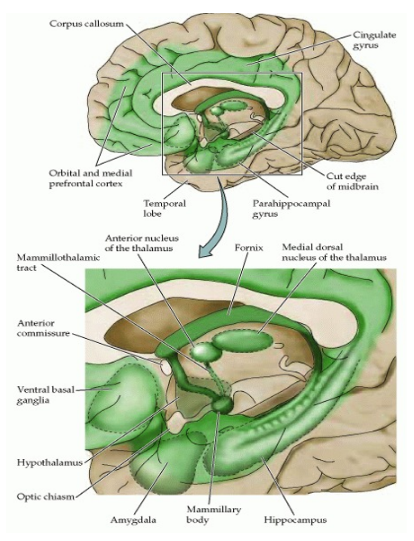
Another way to view the limbic system is dividing it into: Limbic Cortex (Cingulate gyrus, and parahippocampal gyrus), Hippocampal Formation (The dentate gyrus, Hippocampus, Subicular Complex), Amygdala, Septal area, and Hypothalamus (RajMohan & Mohandas, 2007).
These structures are richly connected with each other through variety of neural pathways. Also, all of these connections have extensive fibers pathways that projects to the hypothalamus and multiple sites of brain stem that are involved with the regulation of the internal organs of the body (Neuroanatomy: an Illustrated Colour Text - 6th Edition, n.d.).
In term of functions, generally, the limbic system plays a pivotal role in various processes relating to cognition and behavior including emotions, feeling pleasure, certain forms of memory, learning, motivation, and social processing. Also, the limbic system is regarded as an integral system that operates by influencing the autonomous and endocrine functions (R.L.Isaacson, 2001).
The diseases involving the limbic system can be divided into three categories; diseases in which the limbic system is more or less selectively involved, such as limbic encephalitis, herpes simplex encephalitis, diseases in which the limbic system is predominantly involved, such as, holoprosencephaly, Alzheimer's disease, Pick's disease, hippocampal sclerosis, and vascular diseases of the hippocampal formation; and diseases in which the limbic system is randomly involved, such as various types of neoplasms and vascular and inflammatory lesions (C M Shaw 1, 1997).
An example of the first category is limbic encephalitis (LE), a term that was first described by Brierley et all in 1960 as he reported 3 patients with subacute encephalitis that is mainly involving the limbic areas. Patients usually present with severe progressive short memory deficit, seizures, and psychiatric symptoms (Tüzün & Dalmau, 2007). Two of the patients had bronchial carcinoma, and as the concept of limbic encephalitis expanded, a new entity recognized as paraneoplastic limbic encephalitis (PLE) has evolved. Patient with PLE was noted to have antineuronal antibodies, including anti-Hu and anti-Ta/Ma2, which support the hypothesis that this disease has some autoimmune component (Yuasa T, 2010). In Japan, since 1990, increasing number of non – herpetic acute limbic encephalitis cases were reported. Some of these cases have an autoantibody to GluRepsilon2 (NR2B). GluRepsilon2 is a subunit of the N-methyl-D-aspartate (NMDA) glutamate receptor found in the limbic forebrain. The pathophysiological role of this antibody aid in formulating the concept of autoantibody-mediated acute reversible LE (AMED-ARLE). These variable presentations led to categorizing LE into 3 categories: limbic encephalitis caused by virus infection, autoantibody-mediated limbic encephalitis (AMLE) as in PLE, and limbic encephalitis with autoimmune disease as in AMED-ARLE (Yuasa T, 2010).
A famous example of limbic encephalitis is patient Roger, in whom the infection resulted in massive bilateral limbic system destruction, including the hippocampus, amygdala, parahippocampal gyrus, temporal poles, orbitofrontal cortex, basal forebrain, anterior cingulate cortex, and insular cortex.
He was found unconscious and diagnosed with type 1 virus encephalitis at the age of 28. After a nine-day coma, Roger’s condition stabilized, and he slowly emerged from the coma, completely disoriented. This LE left him with severe amnesia, anosmia, and ageusia. Moreover, Roger’s insight about his condition was impaired and he exhibit total anosognosia. Also, he was noted to have a voracious appetite with willingness to eat unstoppable, disturbed social behavior, and being constantly happy. However, Roger has preserved his above average IQ, normal attention, working memory, and executive function (Feinstein et al., 2010).
Anterograde amnesia is characterized by deficit in the ability to acquire new information and impaired consolidation and storage of the short-term memory. In this case, it most likely results from the destruction of hippocampus. As roger’s procedural memory was intact, this suggests that a different brain area is responsible for this function (Cipolotti & Bird, 2006).
Anosmia and ageusia can be partially explained by knowing that essential parts of the olfactory pathway are located within the limbic system. Essential olfactory information from the cortex is projected to the amygdala, hippocampus, nucleus accumbens, and hypothalamus. It is possible that structural/ functional disturbances to the limbic system as happening in LE can lead to olfactory and gustatory dysfunction (Geran et al., 2019).
Moreover, Roger was noted to have abnormal appetite as Amygdala was affected which plays a major role in food choice, eating behavior, and emotional modulation of food intake. Two nuclei are important in similar cases; the lateral nucleus of the hypothalamus which is the center for control of feeding, and ventromedial nucleus which functions as the satiety center (Ganong, 2003).
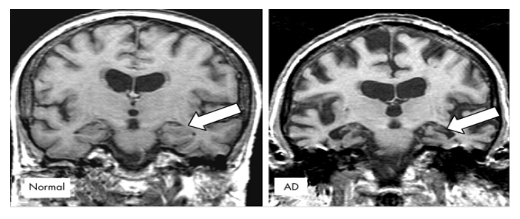
Alzheimer's disease (AD) is another example in which the limbic system is predominantly involved. AD is the most common form of dementia in elderly. It is irreversible brain disorder with wide range of clinical manifestations including memory and language disturbances, visuospatial disorientation, and impaired higher executive functions (Soldan et al., 2016). Although cortical brain has been conventionally associated with Alzheimer's disease, other areas of the brain, notably the hippocampus and amygdala, are involved as well (Hooper & Vogel, 1976). Hippocampal marked volume loss has been recognized as a hallmark of cognitive impairment in Alzheimer's disease. The severity of hippocampal involvement exceeds the involvement elsewhere in the brain (Haque et al., 2019) (Figure 2). Senile plaques and neurofibrillary tangles of the hippocampus can be visualized more readily. Also, senile plaques and neurofibrillary tangles can be visible throughout the cerebral cortex and basal ganglia. Atrophy of the amygdala was noted, and secondary atrophy of the fornix can be seen in chronic cases as well (Hooper & Vogel, 1976). As the dementia progressed, AD patients showed more severe wide spread atrophy of gray matter areas that is more pronounced in the bilateral hippocampus, parahippocampal gyrus, and amygdala (Li et al., 2016). A hallmark of AD is episodic memory loss, which is a type of declarative memory that is very sensitive to age and severely disrupted in AD (Tromp et al., 2015). Another noted phenomenon was that patients with AD have impaired emotional enhancement of memory following emotional stimuli. On the contrary, in neurologically intact individuals, emotional stimuli is associated with enhanced memory (Hamann et al., 2000).
As illustrated by above, hippocampus plays major role in memory processing (Eichenbaum, 2017). Since long, hippocampus has been considered as a central structure for episodic memory encoding, consolidation, and retrieval (Li et al., 2016).
Additionally, integrity of the amygdala is essential for the emotional memory. Also, the interaction between the amygdala, and other brain areas, such as the hippocampal formation, prefrontal cortex, sensory neocortex, striatum, and hypothalamic–pituitary–adrenal axis is crucial as well for the emotional memory (Li et al., 2016).
Indeed, Both amygdala and hippocampus atrophied early in the course of disease and patient may present with memory disturbance years before he is being officially diagnosed with AD (Ortner et al., 2016)(Setti et al., 2017).
Finally, diseases in which the limbic system is randomly involved, such as neoplasms. It has been known since long time that brain tumors have a high incidence of mental abnormalities, including personality changes, behavioral disturbances, emotional defects, and reduced intellectual abilities (Malamud, 1967). A variety of tumor growth patterns have been observed in multiple areas of the limbic system. An association between limbic system lesions and psychotic symptoms has been recognized as demonstrated in a case of 26-year-old Male who developed at age of 13 spells that was accompanied by variable psychiatric symptoms, feeling of numbness, and hallucinations. He was initially diagnosed with petit mall epilepsy and was treated with anticonvulsants. However, patient psychiatric symptoms evolved to hallucinations and delusions which led to the diagnosis of schizophrenia and multiple admissions to a psychiatric institute. Later at autopsy, a tumor was found that was virtually restricted to the left anterior hippocampal region, largely involving the uncus-amygdaloid area and diminishing towards the hippocampus (Malamud, 1967).
Another case of a 19-year-old male who was diagnosed with chronic convulsive disorder at the age of 9 as he experienced grand mal attacks that were accompanied by jerking of the left extremities and inability to speak. Later, he received the diagnosis of depression, anxiety, suicidal and paranoid tendencies as he was suffering from personality changes with emotional tension, increasing withdrawal, aggressive behavior, and negativism. Autopsy revealed a small cystic tumor in the right hippocampal gyrus, compressing the hippocampal formation but not involving the amygdala, on the lateral side of which a massive hemorrhage had occurred (Malamud, 1967).
The above-mentioned cases represent intracranial tumors that involve the limbic system with predominant psychotic symptoms which confirm the generally accepted view that this system does play a significant role in emotions and behavioral expression. Aggressive and impulsive behavior in patients can be explained by deficiency in informational and emotional processing because of neural circuits destruction in the prefrontal and temporal-limbic regions (RajMohan & Mohandas, 2007) (Malamud, 1967).
Moreover, affected cases had seizure which is usually caused by temporal lobe involvement and hippocampal sclerosis. Hippocampal sclerosis with additional involvement of the amygdala and parahippocampal gyrus is termed mesial temporal sclerosis (MTS). It is assumed that MTS is not limited to the medial temporal lobe, but rather it represents a limbic system disorder (Jo et al., 2019).
In conclusion, the limbic system is defined as the brain networking system that is involved in our behavioral responses, emotional drives, and memory formation. Neurological destruction to the limbic system can lead to myriad of clinical manifestations, such as epilepsy, dementia, etc. Moreover, despite the evolving understanding of the limbic system and historical advancement, more research for deeper understanding of the complex structure/function, and associated diseases is highly encouraged.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
